DENTAID Oral Health
News for pharmacy professionals
Gum Care on teeth and implants
05 Sep 2012

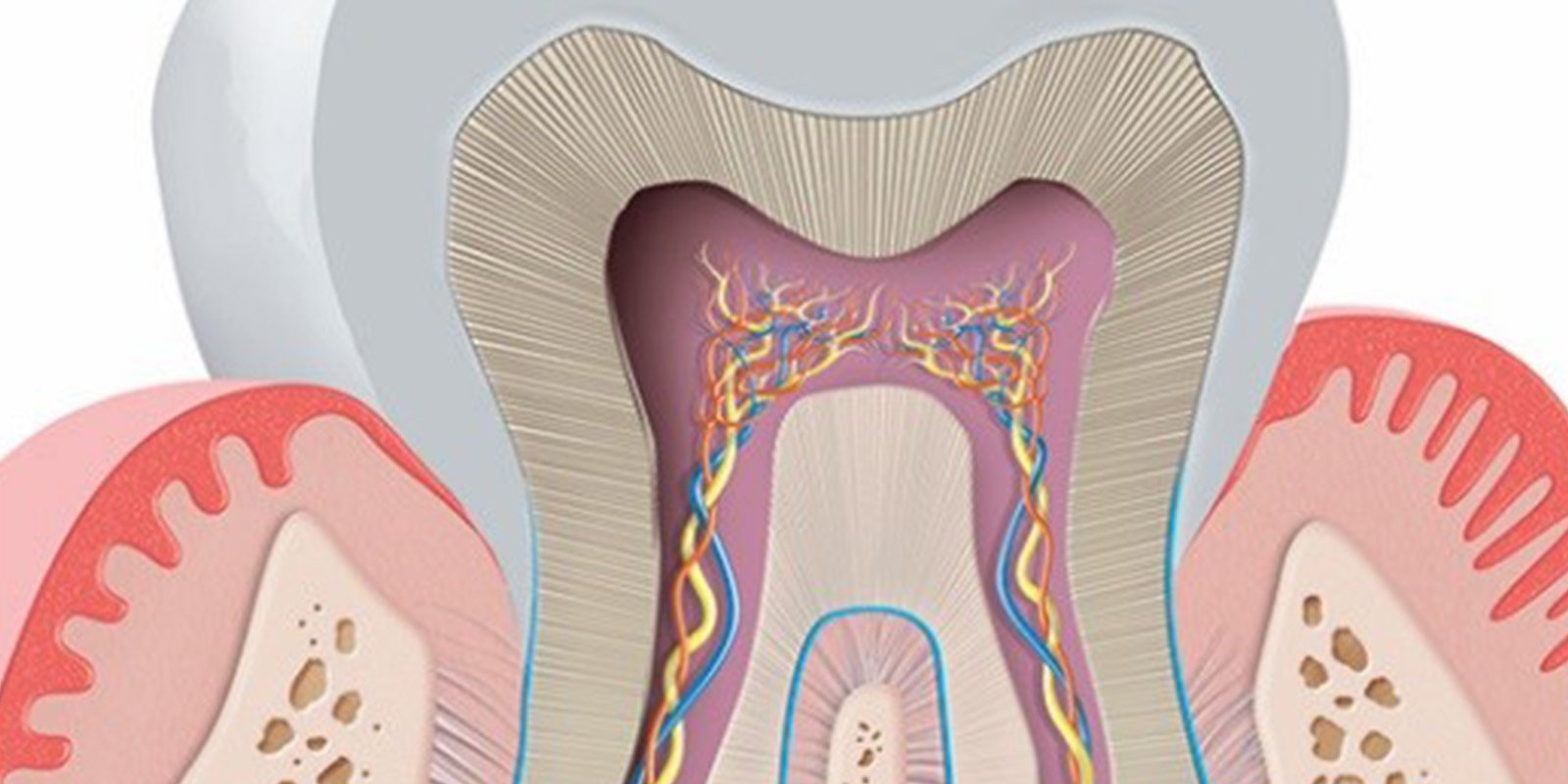
The oral cavity, being an open and dynamic ecosystem, is exposed to numerous factors that regulate microbial composition. Altering the balance of the mouth results in the possible occurrence of gum disease by accumulation of microorganisms that form the biofilm oral (dental plaque).
A gum health conditions should not have swelling or bleeding. If
this condition occurs, it may be because the patient has gum disease,
which can develop on teeth (gingivitis and periodontitis) or dental
implant (peri-implant mucositis and peri). The main causal agent is the accumulation of plaque (oral biofilm).
Gingivitis is characterized by swelling and bleeding of the gums. Usually
redness, swelling and bleeding of the gums, without allowing it to
affect the tissues that support the teeth (periodontium). This condition is reversible, but if left untreated can progress and develop into periodontitis.
Periodontitis
is characterized by redness, swelling, bleeding, gum recession, tooth
mobility and loss of alveolar bone that supports the teeth, and may lead
to tooth loss.
Furthermore, the lining is formed around implants shares similarities with the gum which forms around teeth. As
the periodontal tissue, peri-implant soft tissues have a function of
protection against external environmental aggressions such as
microorganisms. Periimplant
mucosal inflammatory response presents a different, so that after the
oral biofilm accumulation of extension of the inflammation may become
deeper. Therefore,
peri-implant tissues have less capacity to respond to the aggression of
oral biofilm compared to the periodontal tissues.
The
presence of microorganisms on the surface of dental implants occurs
rapidly after exposure to the oral cavity, being able to produce
peri-implant disease (periimplant mucositis and periimplantitis).
Periimplant mucositis is an inflammatory lesion is produced in the mucous membrane which surrounds an implant. The
most common features are: edema, redness and hyperplasia of the mucosa,
bleeding (Ikeda-Artacho et al. 2007) without loss of surrounding bone. The
continued presence of plaque (oral biofilm) on implants induce this
inflammatory reaction and, if not treated properly, can evolve
periimplantitis.
Periimplantitis
is an inflammatory lesion of the mucous membrane which surrounds an
implant in function associated with the loss of supporting bone (Zitmann
and Berglundh 2008). The
injuries are poorly encapsulated periimplantitis, extending to the
marginal bone tissue and, if they advance, they can cause the loss of
the implant.
Prevention and treatment
The
prevention and treatment of periodontal and peri-implant these diseases
should focus on the implementation of anti-infective measures. The
goal is to get the mechanical disintegration plaque (oral biofilm) and
reducing bacteria that cause diseases to levels compatible with health. This requires performing combined treatments that include mechanical and chemical treatment. The mechanical treatment destructured plaque (oral biofilm), however, presents certain limitations in patients who did not.
Therefore, the use of an adjuvant is indispensable as antiseptics chemical mechanical treatment in biofilm control.
Of
these it is known that bisguanidinas antiseptics such as chlorhexidine,
gold standard of antiseptics (Jones 1997; Quirynen 2005) and quaternary
ammonium compounds such as cetylpyridinium chloride, are effective
agents and antiplaque antigingivitis. Not all chlorhexidine mouthwashes have the same effectiveness as it depends on the formulation. Chlorhexidine
0.12%, in combination with cetylpyridinium chloride 0.05% without
alcohol, is indicated in specific situations such as periodontitis
(Herrera et al. 2003) and periimplantitis (Garcia and Lopez 2010). Numerous
scientific publications is endorsed as the most effective antiseptic
formulation (Quirynen et al. 2001, Herrera et al. 2003).
Chlorhexidine
at low concentrations in combination with 0.05% cetylpyridinium
chloride can be 0.05% of the daily recommended to monitor the recurrence
of periodontal disease, particularly in patients who did not adhere as
well as in situations less complex (Escribano et al. 2010).
Cetylpyridinium chloride is an inhibitor of plaque classified by the FDA under the category I (safe and effective). Recommend
its use on a daily basis to prevent gingivitis and peri-implant
mucositis (Dr. Augustine Homes: 'peri-implant mucositis: how can you
prevent it?', I SEPADENTAID Symposium 2012).
That
is why efforts should focus on maintaining the health of teeth and
implants or, which is, in preventing the onset of periodontal and
peri-implant diseases, which will aim to prevent inflammation and
infection of the and
peri-implant dental tissues and prevent the formation of a pathogenic
biofilm, thus minimizing the risk of treatment failure and periodontal
implants.
Bibliography
1. Escribano M., Herrera D., S. Morante, Teughels W., Quirynen M., Sanz M. (2010). 'Efficacy
of a low-concentration chlorhexidine mouth rinse in noncompliant
periodontitis patients attending a supportive periodontal care program: a
randomized clinical trial'. Journal of Clinical Periodontology, 37: 266-275.
2. D. Garcia and M. Lopez (2010). 'Drug Interactions in periimplantitis'. Journal of the American Dental Association, Vol.5 No.1.
3. Herrera D, Roldán S., I. Santacruz, S. Santos, Masdevall M., Sanz M. (2003). 'Differences
in antimicrobial activity of four commercial 0.12% chlorhexidine
mouthrinse Formulations: an in vitro contact test and salivary bacterial
counts study'. Journal of Clinical Periodontology, April, 30 (4): 307-14.
4. Ikeda-Artacho M., Ceccarelli, J. Street, D. Casalino Proaño- (2007) 'Periimplantitis and peri-implant mucositis.' Herediana Stomatology Magazine, 17 (2): 90-98.
5. Jones C. (1997). 'Chlorhexidine: is it still the gold standard?'. Periodontology 2000, 15, 55-62.
6. Quirynen M., Avontroodt P., Peeters W, Pauwels M, Coucke W, van Steenberghe D. (2001). 'Effect of different chlorhexidine mouthrinses on the Formulations in novo plaque formation.' Journal of Clinical Periodontology, 28: 1127-36
7. Quirynen M., C. Soers, Desnyder M., C. Dekeyser, M. Pauwels, D. van Steenberghe (2005). 'A 0.05% cetyl pyridinium chloride/0.05% chlorhexidine mouthrinse During maintenance phase after initial periodontal therapy'. Journal of Clinical Periodontology, 32: 390-400.
8. Zitzmann N. and T. Berglundh (2008). 'Definition and Prevalence of periimplant diseases'. Journal of Clinical Periodontology, 35 (Suppl. 8): 286-291.
RELATED ARTICLES

18 Nov 2021
Laboratory studies prove that CPC in mouthwashes is effective against different variants of SARS-CoV-2 thanks to its mechanism of action
INTRODUCTION The oral cavity is a route of entry, infection and transmission of microorganisms, including the SARS-CoV-2 coronavirus. Several…
11 Apr 2019
PERIODONTAL DISEASE EXPLAINED FOR THE PHARMACIST
Periodontal disease, aka gum disease, is a set of chronic infectious diseases that affect the periodontium, causing inflammation and/or subsequent…

15 Jan 2019
ORAL HEALTH IN ADULTS OVER AGE FIFTY
As the years go by, the mouth undergoes both anatomical and physiological changes. These changes, together with poor oral hygiene and certain…
Sign up for the DENTAID Oral Health newsletter
Sign up for the newsletter
Sign up for the DENTAID Oral Health newsletter
| Data controller | DENTAID, S.L. LABORATORIOS DE PREVENCIÓN E HIGIENE BUCAL, SLU (“PHB”). |
|---|---|
| Purpose of data processing | To respond to a query from the interested party with the advice of a specialist. |
| Legitimisation of data processing | Your consent to process your personal data. |
| Recipients of disclosure or transfer | Data is not disclosed or transferred internationally. |
| Rights of the interested persons | To access, rectify and delete their data, and to exercise other rights as set out in the additional information. |
| Additional information | You can consult additional and detailed information on data protection at this link. |
Sign up for the DENTAID Oral Health newsletter
| Data controller | DENTAID, S.L. LABORATORIOS DE PREVENCIÓN E HIGIENE BUCAL, SLU (“PHB”). |
|---|---|
| Purpose of data processing | To respond to a query from the interested party with the advice of a specialist. |
| Legitimisation of data processing | Your consent to process your personal data. |
| Recipients of disclosure or transfer | Data is not disclosed or transferred internationally. |
| Rights of the interested persons | To access, rectify and delete their data, and to exercise other rights as set out in the additional information. |
| Additional information | You can consult additional and detailed information on data protection at this link. |